Name/Title
Life insurance certificate from The Order of Railroad TelegraphersEntry/Object ID
1986.18.38Scope and Content
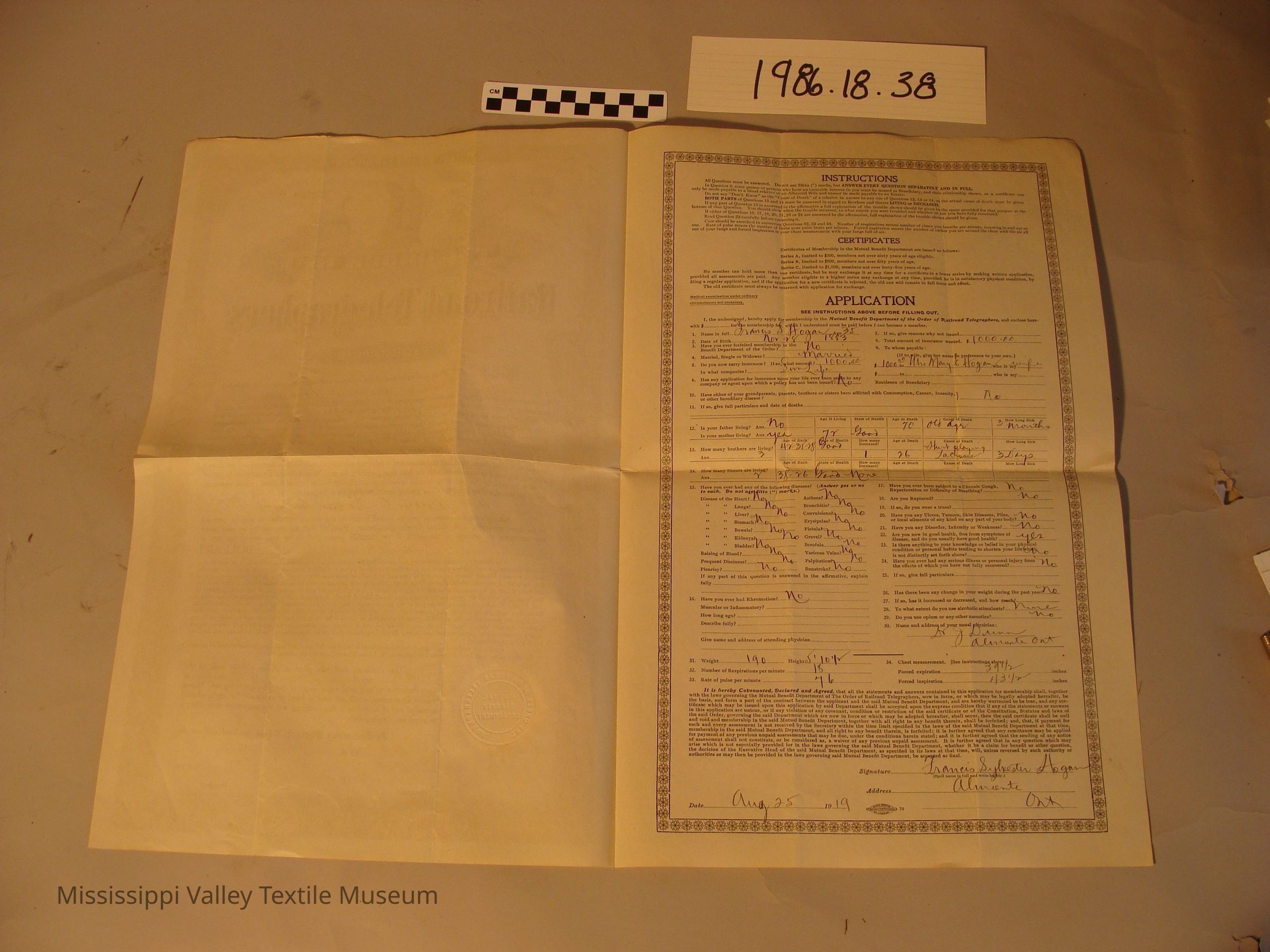
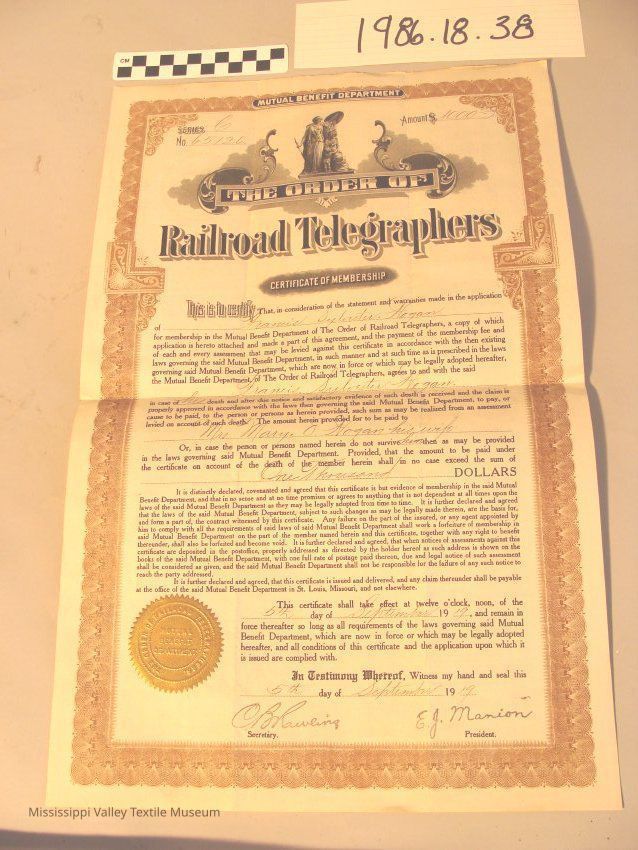
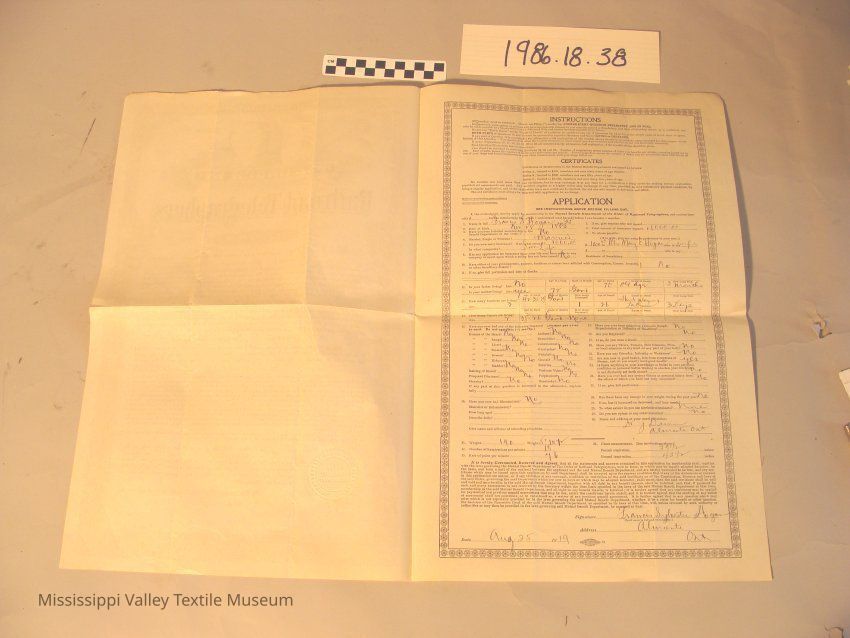
Large 2 page life insurance agreement from The Order of the Railroad Telegraphers for Francis Sylvester Hoganand of Almonte. It states that in case of death his wife, Mrs. Mary E. Hogan will recieve no more than one thousand dollars. Page one is the certificate, the second page is the application which includes medial history.
Transcription of the artifact is as follows:
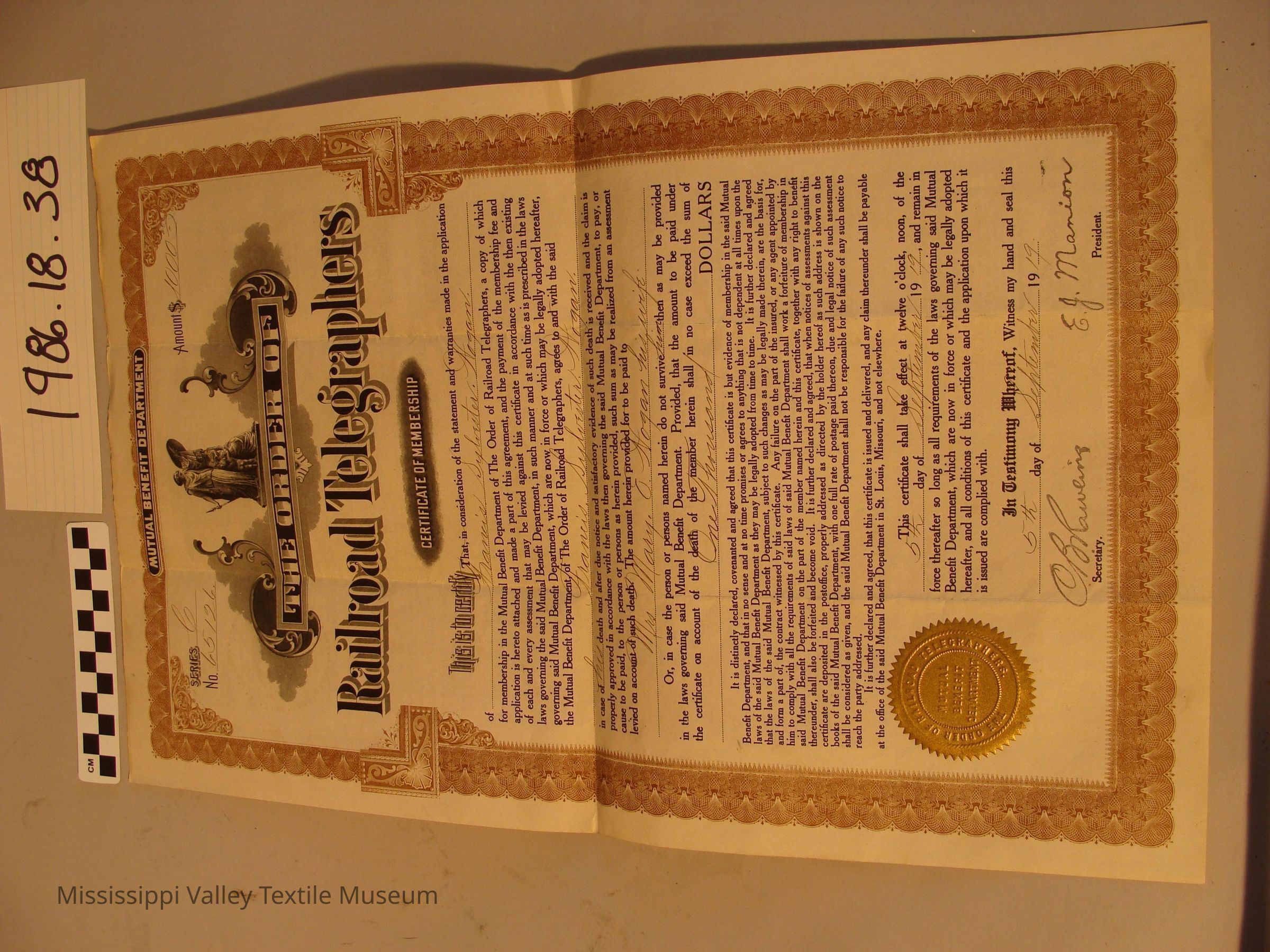
[the following is written on the front side of the document once it has been folded open]
MUTUAL BENEFIT DEPARTMENT
SERIES C Amount $1000
No. 65126
THE ORDER OF
Railroad Telegraphers
CERTIFICATE OF MEMBERSHIP
This is to certify That, in consideration of the statement and warranties made in the application of Francis Sylvester Hogan for membership in the Mutual Benefit Department of The Order of Railroad Telegraphers, a copy of which application is hereto attached and made a part of this agreement, and the payment of the membership fee and of each and every assessment that may be levied against this certificate in accordance with the then existing laws governing said Mutual Benefit Department, which are now in force or which may be legally adopted hereafter, the Mutual Benefit Department, of The Order of Railroad Telegraphers, agrees to and with the said Francis Sylvester Hogan. In case of his death and after due to notice and satisfactory evidence of such death is received and the claim is properly approved in accordance with the laws then governing the said Mutual Benefit Department, to pay, or cause to be paid, to the person or persons as herein provided, such sum as may be realized from an assessment levied on account of such death. The amount herein provided for to be paid to Mrs Mary E Hogan his wife Or, in case the person or persons named herein do not survive him then as may be provided in the laws governing said Mutual Benefit Department. Provided, that the amount to be paid under the certificate on account of the death of the member herein shall in no case exceed the sum of One Thousand DOLLARS
It is distinctly declared, covenanted and agreed that this certificate is but evidence of membership in the said Mutual Benefit Department, and that in no sense and at no time promises or agrees to anything that is not dependent at all times upon the laws of the said Mutual Benefit Department as they may be legally adopted from time to time. It is further declared and agreed that the laws of the said Mutual Benefit Department, subject to such changes as may be legally made therein, are the basis for, and form a part of, the contract witnessed by this certificate. Any failure on the part of the insured, or any agent appointed by him to comply with all the requirements of said laws of the said Mutual Benefit Department shall work a forfeiture of membership in said Mutual Benefit Department on the part of the member named herein and this certificate, together with any right to benefit thereunder, shall also be forfeited and become void. It is further declared and agreed, that when notices of assessments against this certificate are deposited in the postoffice, properly addressed as directed by the holder hereof as such address is shown on the books of the said Mutual Benefit Department, with one full rate of postage paid thereon, due and legal notice of such assessment shall be considered as given, and the said Mutual Benefit Department shall not be responsible for the failure of any such notice to reach the party addressed.
It is further declared and agreed, that his certificate is issued and delivered, and any claim thereunder shall be payable at the office of the said Mutual Benefit Department in St Louis, Missouri, and not elsewhere.
This certificate shall take effect at twelve o’clock, noon, of the 5th day of September 1919, and remain in force thereafter so long as all requirements of the laws governing said Mutual Benefit Department, which are now in force or which may be legally adopted hereafter, and all conditions of this certificate and the application upon which it is issued are complied with.
In Testimony Whereof, Witness my hand and seal this 5th day of September 1919
C.B. Rawling Secretary. E.J. Manion President.
[the following is written on the inside of the document when folded open]
INSTRUCTIONS
All Questions must be answered. Do not use Ditto (“) marks, BUT ANSWER EVERY QUESTION SEPARATELY AND IN FULL. In Question 9, some person or persons who have an insurable interest in you must be named as Beneficiary, and their relationship shown, as a certificate can only be made payable to a blood relative or an Affianced Wife and cannot be made payable to an Estate. Do not say “Don’t Know” as the “Cause of Death” of a relative in answer to any one of Questions 12, 13 or 14, as the actual cause of death must be given. BOTH PARTS of Questions 13 and 14 must be answered in regard to Brothers and Sisters LIVING or DECEASED. If any part of Question 15 is answered in the affirmative a full explanation of the trouble shown should be given in the space provided for that purpose at the bottom of that Question. You should show when the trouble occurred, to what extent you were troubled and whether or not you have fully recovered. If either of Questions 16, 17, 18, 20, 21, 23 or 24 are answered in the affirmative, full explanation of the trouble shown should be given. Read Question 22 carefully before answering it. Care should be exercised in answering Questions 32, 33 and 34. Number of respirations means number of times you breathe per minute, counting in and out as one. Rate of pulse means the number of times your pulse beats per minute. Forced expiration means the number of inches you are around the chest with the air all out of your lungs and forced inspiration is your chest measurement with your lungs full of air.
CERTIFICATES
Certificates of Membership in the Mutual Benefit Department are issued as follows:
Series A, limited to $300, members not over sixty years of age eligible.
Series B, limited to $500, members not over fifty years of age.
Series C, limited to $1,000, members not over forty-five years of age.
No member can hold more than one certificate, but he may exchange it at any time for a certificate in a lower series by making written application, provided all assessments are paid. Any number eligible to a higher series may exchange at any time, provided he is in satisfactory physical condition, by filing a regular application, and if the application for a new certificate is rejected, the old one will remain in full force and effect.
The old certificate must always be returned with application for exchange.
Medical examination under ordinary circumstances not necessary.
APPLICATION
SEE INSTRUCTIONS ABOVE BEFORE FILLING OUT.
I, the undersigned, hereby apply for membership in the Mutual Benefit Department of the Order of Railroad Telegraphers, and enclose herewith $____ for the membership fee, which I understand must be paid before I can become a member.
Name in full James S Hogan Age 35
Date of Birth Nov 28 1883
Have you ever forfeited membership in the Benefit Department of the Order? No
Married, Single or Widower? Married
Do you now carry insurance? If so, what amount? 1000.00 In what companies? SunLife
Has any application for insurance upon your life ever been made to any company or agent upon which a policy has not been issued? No
If so, give reasons why not issued___
Total amount of insurance wanted. $1000.00
To whom payable:
(If to wife, give her name in preference of your own.)
$1000 to Mrs Mary R Hogan who is my wife
$___ to ______ who is my ____
Residence of Beneficiary _____
Have either of your grandparents, parents, brothers or sisters been afflicted with Consumption, Cancer, Insanity, or other hereditary disease? No
If so, give full particulars and date of deaths_________
Is your father living? Ans. No [the following are headings for a table] Age if Living State of Health Age at Death [“70” is written here] Cause of Death [“old age” is written] How Long Sick [“3 months” is written]
Is your mother living? Ans. Yes 72 Good
How many brothers are living? Ans. 3 [the following are headings for a table] Age of Each [“42 35 28” is written] State of Health [“good” is written] How many Deceased? [“1” is written] Age at Death [“26” is written] Cause of Death [“Hurt playing Lacrosse” is written] How Long Sick [“32 days” is written]
How many Sisters are living? Ans. 2 [the following are headings for a table] Age of Each [“28, 26” is written] State of Health [“good” is written] Ho many Deceased [“none” is written] Age at Death Cause of Death How Long Sick
Have you ever had any of the following diseases? (Answer yes or no to each. Do not use ditto (“) marks.)
Disease of the Heart? No Asthma? No
“ “ Lungs? No Bronchitis? No
“ “ Liver? No Convulsions? No
“ “ Stomach? No Erysipelas? No
“ “ Bowels? No Fistula? No
“ “ Kidneys? No Gravel? No
“ “ Bladder? No Scrofula? No
Raising of Blood? No Varicose Veins? No
Frequent Dizziness? No Palpitation? No
Pleurisy? No Sunstroke? No
If any part of this questions is answered in the affirmative, explain fully ______
Have you ever had Rheumatism? No
Muscular or inflammatory?____
How long ago?_____
Describe fully?_____
Give name and address of attending physician_______
Have you ever been subject to a Chronic Cough, Expectation or Difficulty of Breathing? No
Are you Ruptured? No
If so, do you wear a truss? _____
Have you any Ulcers, Tumors, Skin Diseases, Piles, or local ailments of any kind on any part of your body? No
Have you any Disorder, Infirmity or Weakness? No
Are you now in good health, free from symptoms of disease, and do you usually have good health? Yes
Is there anything to your knowledge or belief in your physical condition or personal habits tending to shorten your life which is not distinctly set forth above? No
Have you ever had any serious illness or personal injury from the effects of which you have not fully recovered? No
If so, give full particulars_____
Has there been any change in your weight during the past year No
If so, has it increased or decreased, and how much?____
To what extent do you use alcoholic stimulants? None
Do you use opium or any other narcotics? No
Name and address of your usual physician:
Dr J Dunn
Almonte Ont
Weight 190 Height 5’10 ½
Number of Respirations per minute 18
Rate of pulse per minute 76
Chest measurement. [See instructions above.]
Forced expiration 39 ½ inches
Forced inspiration 43 ½ inches
It is hereby Covenanted, Declared and Agreed, that all the statements and answers contained in this application for membership shall, together with the laws governing the Mutual Benefit Department of the Order of Railroad Telegraphers, now in force, or which may be legally adopted hereafter, be the basis, and form a part of the contract between the applicant and the said Mutual Benefit Department, and are hereby warranted to be true, and any certificate which may be issued upon this application by said Department shall be accepted upon the express condition that if any of the statements or answers in this application are untrue, or if any violation of any covenant, condition or restriction of the said certificate or of the Constitution, Statutes and laws of the said Order, governing the said Department which are now in force ot which may be adopted hereafter, shall occur, then the said certificate shall be null and void and membership in the said Mutual Benefit Department, and all right to any benefit therein, is forfeited; and , that if payment for each and every assessmentis not recieed by the secertary within the time limit specified in the laws of the said Mutual Benifit Department at that time, membership ins the said Mutual Benefit Department, and all right to anybenefit therein, is forfeited; it is further agreed that any remittance may be applied for payment of any previous unpaid assessments that may be due, under the conditions herein stated, and it is further agreed that the sending of any notice of assessment shall not constitute, or be considered as, a waiver of any previous unpaid assessment. It is further agreed that in any question which may arise which is not especially provided for in the laws governing the said Mutual Benefit Department, whether it be a claim for benefit or other question, the decision of the Executive Head of the said Mutual Benefit Department, as specified in its laws at that time, will, unless reversed by such authority or authorities as may then be provided in the laws governing said Mutual Benefit Department, be accepted as final.
Signature Francis Sylvester Hogan
Address Almonte Ont
Date Aug 25 1919
[the following is written on the back side of the document when folded open]
MUTUAL BENEFIT DEPARTMENT
THE ORDER OR
Railroad Telegraphers
CERTIFICATE OF MEMBERSHIP
OF
Francis S Hogan
CERTIFICATE NO. 65126.
SERIES C
$1000
BE SURE TO NOTIFY THE SECRETARY OF ANY CHANGE IN YOUR POSTOFFICE ADDRESS. THE DUTY OF THE DEPARTMENT IS FULFILLED AND ITS RESPONSIBILITY CEASES WHEN THE NOTICE IS MAILED.
Written byCollection
AlmonteCataloged By
Paul, NancyLexicon
Legacy Lexicon
Object Name
Certificate, InsuranceArchive Details
Date(s) of Creation
Sep 5, 1919Location
Location
Container
Box 5Shelf
Shelf 19Room
Collections RoomBuilding
M.V.T.M.Category
PermanentDate
November 7, 2023Location
Container
Box 2Shelf
Shelf 7, Shelf 7Room
Collections RoomBuilding
M.V.T.M.Category
PermanentMoved By
Plewes, ColeDate
June 15, 2019Location
Container
Box 5Shelf
Shelf 19, Shelf 19Room
Collections RoomBuilding
M.V.T.M.Category
PermanentMoved By
Plewes, ColeDate
June 15, 2019Location
Container
Archive Box 1Shelf
Shelf 1, Shelf 1Room
Collections RoomBuilding
M.V.T.M.Category
PermanentMoved By
Whit, ElizabethDate
August 7, 2016Category
PermanentGeneral Notes
Note
Status: OK
Status By: Cotter, Ellen
Status Date: 2022-02-08Created By
admin@catalogit.appCreate Date
May 9, 1986Updated By
admin@catalogit.appUpdate Date
November 12, 2023